BLOOD:
Learning Objectives: Lectures, Chapter 12Upon completion of the lectures and this chapter, you should be able to:
- Describe the primary functions of blood.
- Explain the composition of blood.
- Describe the characteristics of centrifuged blood.
- Explain the characteristics of blood plasma.
- List the formed elements of blood.
- Identify the formed elements and the most important functions of each.
- Discuss the structure and function of red blood cells and how red blood cells numbers and hemoglobin content may change to produce anemia.
- Describe ABO and Rh blood typing, the universal donor, the universal recipient, and consequences of receiving the wrong blood type.
- Discuss the structure and function of white blood cells.
- Explain the role of platelets and the steps involved in blood clotting.
- Define the medical terms associated with blood, including hemoglobin, hematocrit, acidosis, serum, antiserum, plasma, formed elements, anemia, sickle cell, polycythemia, erythroblastosis fetalis, Rh factor, leukocytosis, leukopenia, phagocytosis, fibrin, fibrinogen, thrombosis, hemolysis, agglutination.
- Understand the key components and purposes of the following blood tests: CBC, WBC differential, hematocrit, hemoglobin, coagulation time.
- Name the components of blood.
- Describe the structure, characteristics and function of the red blood cells, white blood cells and platelets.
- Identify red blood cells, white blood cells and platelets on blood smear slides.
- Describe the importance of and perform ABO and Rh blood typing on simulated blood.
- Perform an ABO/Rh blood typing cross-match test using simulated "blood" and "antiserum".
- Describe the importance of the following blood tests: differential WBC count, hematocrit, hemoglobin, and coagulation time and the purpose of a CBC.
- Identify the elevations and depressions of white blood cells and the diseases and conditions they are linked with.
- Identify the components of centrifuged blood.
- Understand the structure and function of plasma and serum.
- Discuss the location, size, and position of the heart in the thoracic cavity.
- Identify the heart chambers, valves and sounds.
- Recognize the structural characteristics of the heart.
- Trace the path of blood through the heart and compare the functions of the heart chambers on the right and left sides.
- List the anatomical components of the heart conduction system and discuss the features of a normal electrocardiogram (EKG).
The Blood:
Components of Blood:
Plasma - clear, straw-colored liquid portion of blood.
Formed Elements - dark red and buff-colored portions that include 3 types of blood cells.
- Adult cardiovascular system contains about 5.5 liters of blood.
- When blood is centrifuged, it separates visually into two major components: plasma and formed elements.
- Hematology - the study of blood and blood products and blood diseases
- For more detailed information, feel free to visit my website at www.hematologylearning.weebly.com
Components of Blood:
Plasma - clear, straw-colored liquid portion of blood.
- Constitutes about 55% of whole blood
- Is about 91.5% water
- Is about 8.4% solutes (dissolved minerals and ions and plasma proteins and nutrients, including glucose, amino acids, lipids, blood gases [O2, CO2], electrolytes, hormones, enzymes, and waste products)
Formed Elements - dark red and buff-colored portions that include 3 types of blood cells.
- Constitute about 45% of whole blood
The Blood: Chapter 12The adult cardiovascular system contains about 5.5 liters of blood. When blood is centrifuged, it separates visually into two distinct major components:
Type of Cell:
Scientific Name:
Role and Function:
Red blood cells
Erythrocytes
Erythro = red
Cytes= cells
They carry hemoglobin, which carries iron, which binds and carries oxygen to the tissues of the body. About 33% of the total weight of RBC's is hemoglobin.
Hemoglobin contains a red pigment called heme. This gives blood its red color.
Bright red blood: oxygenated
Dark red blood: deoxygenated.
There are 4.5-5 million per microliter of blood.
They are small an anucleate (contain no nucleus at maturity).
Polycythemia - This is having too many red blood cells, such as at high elevations (moving, traveling) or a genetic type, which puts a person at higher risk for blood clots and strokes.
Poly = many
Cyto = cells
Emia =blood
Anemia - This is having an unusually low number of RBC's or hemoglobin, resulting in iron-deficiency anemia. There are other types of anemia as well. See www.hematologylearning.weebly.com for more information about blood disorders.
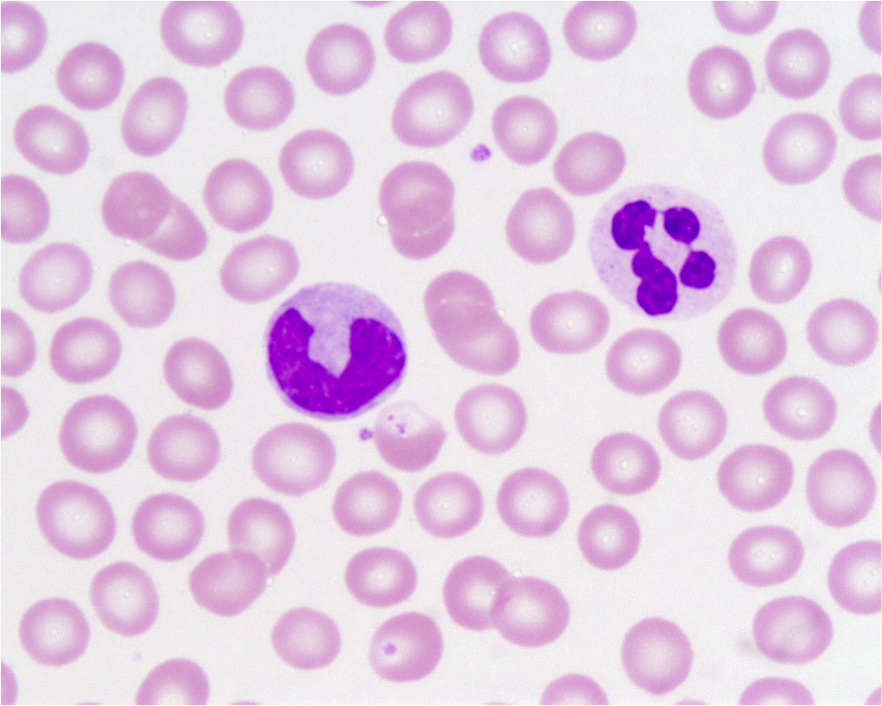
Stain Color - In special Wright's stain or Modified Wright-Giemsa Stain, RBC's look like small, pinkish cells with a small white indentation in the middle, like a "Smartie's" candy.
White blood cells
Leukocytes
Leuko = white
They play a key role in immunity.
There are five types, divided into two categories:
Granulocytes - contain vesicles with granules in the cytoplasm that can be seen after staining.
Leukocytosis - an unusually high number of WBC's, indicating a pathological condition.
Osis = an increase in a pathological condition
Lymphocytosis - an unusually low number of WBC's, which may indicate a pathological condition.
Penia = deficiency
Stain Color - In Wright's Stain or Modified Wright Giemsa Stain, WBC's stain light lavender with a dark blue to dark purple nucleus. They are much larger than RBC's.
PlateletsThrombocytes
Thrombo = clot
They play a key role in blood clotting, or coagulation.
They form from large, multinuclear cells called megakaryocytes.
Mega = large
Karyo = nucleus
Cytes = cells
Megakaryocytes break into small, disc-shaped fragments called platelets.
Platelets do not have nuclei.
Platelets protect the body by forming a platelet plug to stop bleeding when blood vessels rupture.
Platelets become sticky when activated, secreting chemicals that aid in blood clotting.
Thrombocytopenia - deficiency in the number of circulating platelets.
Thrombocytosis - abnormal increase in the number of circulating platelets.
Stain Color - In Wright's Stain or Modified Wright-Giemsa Stain, platelets stain dark purple and are very tiny. They are dispersed amongst the red blood cells and white blood cells.
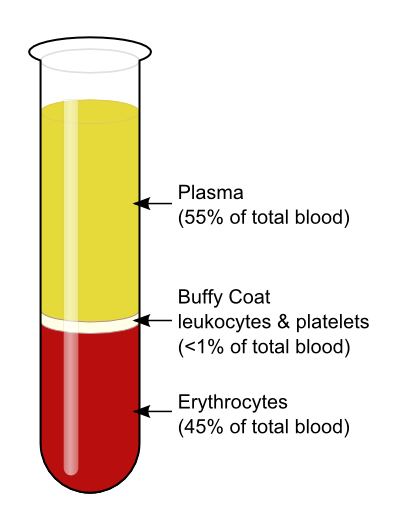
The formed elements constitute about 45% of whole blood volume.
The plasma constitutes about 55% of whole blood volume and is about:
- Plasma - the clear, straw-colored liquid portion of blood
- Formed elements - dark red and buff-colored portions of blood, which include the red blood cells, white blood cells and platelets (cell fragments)
Type of Cell:
Scientific Name:
Role and Function:
Red blood cells
Erythrocytes
Erythro = red
Cytes= cells
They carry hemoglobin, which carries iron, which binds and carries oxygen to the tissues of the body. About 33% of the total weight of RBC's is hemoglobin.
Hemoglobin contains a red pigment called heme. This gives blood its red color.
Bright red blood: oxygenated
Dark red blood: deoxygenated.
There are 4.5-5 million per microliter of blood.
They are small an anucleate (contain no nucleus at maturity).
Polycythemia - This is having too many red blood cells, such as at high elevations (moving, traveling) or a genetic type, which puts a person at higher risk for blood clots and strokes.
Poly = many
Cyto = cells
Emia =blood
Anemia - This is having an unusually low number of RBC's or hemoglobin, resulting in iron-deficiency anemia. There are other types of anemia as well. See www.hematologylearning.weebly.com for more information about blood disorders.
Stain Color - In special Wright's stain or Modified Wright-Giemsa Stain, RBC's look like small, pinkish cells with a small white indentation in the middle, like a "Smartie's" candy.
White blood cells
Leukocytes
Leuko = white
They play a key role in immunity.
There are five types, divided into two categories:
Granulocytes - contain vesicles with granules in the cytoplasm that can be seen after staining.
- Neutrophils
- Eosinophils
- Basophils
- Lymphocytes
- Monocytes and Macrophages
Leukocytosis - an unusually high number of WBC's, indicating a pathological condition.
Osis = an increase in a pathological condition
Lymphocytosis - an unusually low number of WBC's, which may indicate a pathological condition.
Penia = deficiency
Stain Color - In Wright's Stain or Modified Wright Giemsa Stain, WBC's stain light lavender with a dark blue to dark purple nucleus. They are much larger than RBC's.
PlateletsThrombocytes
Thrombo = clot
They play a key role in blood clotting, or coagulation.
They form from large, multinuclear cells called megakaryocytes.
Mega = large
Karyo = nucleus
Cytes = cells
Megakaryocytes break into small, disc-shaped fragments called platelets.
Platelets do not have nuclei.
Platelets protect the body by forming a platelet plug to stop bleeding when blood vessels rupture.
Platelets become sticky when activated, secreting chemicals that aid in blood clotting.
Thrombocytopenia - deficiency in the number of circulating platelets.
Thrombocytosis - abnormal increase in the number of circulating platelets.
Stain Color - In Wright's Stain or Modified Wright-Giemsa Stain, platelets stain dark purple and are very tiny. They are dispersed amongst the red blood cells and white blood cells.
The formed elements constitute about 45% of whole blood volume.
The plasma constitutes about 55% of whole blood volume and is about:
- 91.5% water
- 8.5% solutes
- Plasma proteins (albumin, globulins)
- Nutrients: glucose, amino acids, lipids
- Blood gases: O2 , CO2
- Electrolytes
- Hormones
- Enzymes
- Waste Materials
- The study of blood is called HEMATOLOGY
- Hematologic Tests are performed to study plasma and formed elements of blood and are very useful diagnostic tools since the composition of blood reflects the general health of an individual and can detect normal and abnormal body functions and conditions
- Blood must be handled in a safe manner, including the wearing of a lab coat or apron, gloves and safety glasses or goggles and working slowly and carefully and observing all precautions for disposal of human waste
- All soiled glassware should be soaked in bleach immediately after use for at least 30 minutes prior to autoclaving (sterilizing)
- All disposable items, including cotton balls, gauze, alcohol swabs, paper towels, lancets, etc... should be placed in a disposable red/orange, biohazard autoclave bag so it can be sterilized prior to disposal
- Soiled sharps need to be disposed of in designated and labeled sharps containers
Blood typing is critical for the following:
- Blood transfusions
- Organ transplants
- Bone marrow transplants
- Maternal-fetal compatibility
- Genetic studies
- Forensic studies
- Legal medicine
- Anthropology
Important Terminology:
- Antigen - a substance that will react to a specific antibody to produce an immune response.
- Antibody - plasma proteins that combine with a specific antigen to inhibit or destroy it
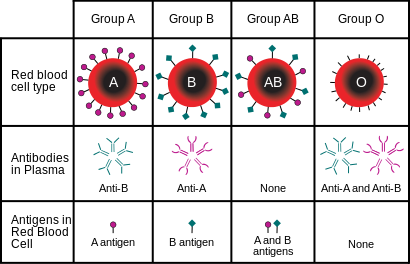
- ABO system - there are two types of antigens (A and B) that can be present as surface membrane molecules on red blood cells.
- Type A blood - only the A antigen is present on the red blood cell membrane
- Have anti-B antibodies in their plasma
- Type B blood - only the B antigen is present on the red blood cell membrane
- Have anti-A antibodies in their plasma
- Type AB blood - BOTH the A AND the B antigen are present on the red blood cell membrane; This type is called the universal recipient because it can receive blood from ANY blood type
- Have NO antibodies against A or B antigens in their plasma so they can receive blood from type A, B, AB or O
- Type O blood - NEITHER A NOR B antigens are present on the red blood cell membrane; This type is called the universal donor and can donate blood to ANY blood type
- Have BOTH anti-A AND anti-B antigens in their plasma so they can only receive type O blood
- ABO antibodies - appear in babies' blood a few months after birth and do not cross the placenta because they are too big.
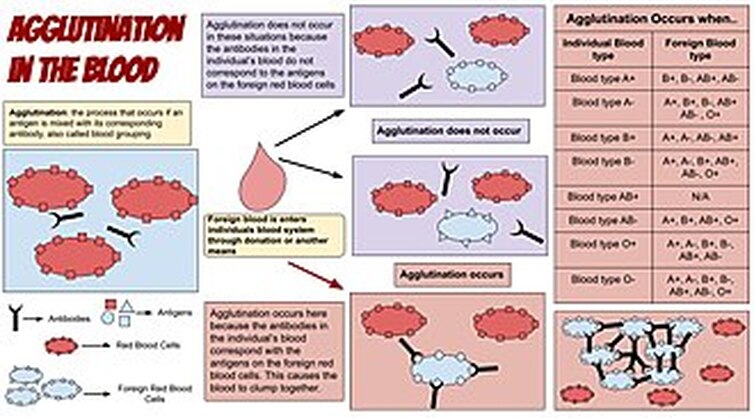
- Agglutinate - means to clump or clot; this happens when people receive the wrong blood type, so their antigens cross-link with antibodies, which cause them to stick together and activate another plasma protein that attaches to the recipient's red blood cells and causes them to swell up and hemolyze (burst), releasing hemoglobin that can damage the kidneys and other orgrans.
- Rh blood system - means that the Rh-antigen is present as a surface membrane molecule on the RBC's if Rh-positive (Rh +) and not present if Rh-negative (Rh - ).
- Rh negative - do not have the anti-Rh antibody and do not obtain it unless they are exposed to Rh-antigen from Rh-positive blood through:
- a blood transfusion
- sharing hypodermic needles
- by an Rh-negative mother carrying an Rh-positive fetus since the baby's blood can leak from the placenta into the mother's bloodstream during delivery, causing her body to make Rh-antibodies
- NOTE: The first baby is not affected, but subsequent pregnancies with Rh-positive fetuses can result in the small Rh-antibodies crossing the placenta, cuasing hemolysis in the blood of the fetus in a condition known as hemolytic disease of the newborn.
- Prevention: RhoGAM shots given to Rh-negative mothers carrying Rh-positive fetuses so they will not make Rh-antibodies.
- Rh negative - do not have the anti-Rh antibody and do not obtain it unless they are exposed to Rh-antigen from Rh-positive blood through:
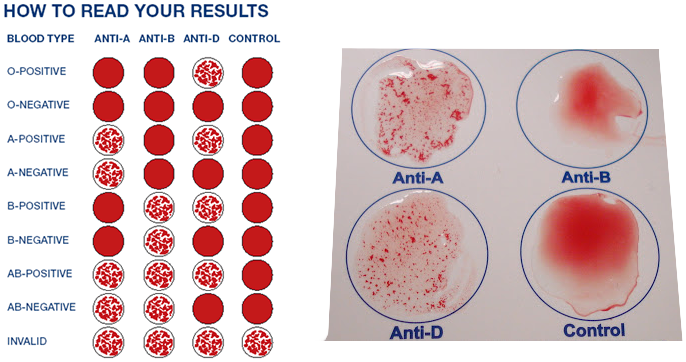
Blood typing is a laboratory test that utilizes antisera containing antibodies against A, B or D (Rh) antigens. Serum (or simulated serum) is blood plasma without clotting proteins. For example, if anti-A serum clumps a particular blood sample, the blood is type A because this indicates that an antibody-antigen complex formed between the A antigens on the red blood cells and the A antibodies in the antiserum.
Complete lab activity 2 using the lab kit mailed to you by Carolina Biological Distance Learning Lab Kits for ABO and Rh Blood Typing. Use appropriate PPE (gloves, goggles, apron) to complete this activity. You will be using simulated blood samples and antisera for this activity. You will be performing this on a card or plate as shown, but I also included pictures I took when working in the lab of other methods used for blood typing, which include the tube test (in test tubes) and the gel test (in gel cards) for comparison.
The Complete Blood Count:
The CBC is a vital diagnostic tool that screens for abnormalities in the number or structure of red blood cells and includes the following components:
The differential WBC count is performed to determine the actual percentage of each of the five types of WBC's in a blood sample. Elevations or depressions in these numbers can indicate various diseases, illnesses, or conditions that need to be further evaluated.
CBCWBCRBCHGBHCTMCVMCHMCHCRDWPLTMPVNEUT%LYMPH%MONO%EO%BASO%NEUT#LYMPH#MONO#EO#BASO#4.5-11.0
4.70-6.1014-1842-5283-9928-3431-3711-15.5150-4507.4-10.449-9022-51.10-130-70-31.5-7.06.70-3.00-1.40-0.80-0.3
x 103/UL
x 106/UL
G/DL%FLPG
%%x 103/UL
FL%%%%%x 103/UL
x 103/ULx 103/ULx 103/ULx 103/UL
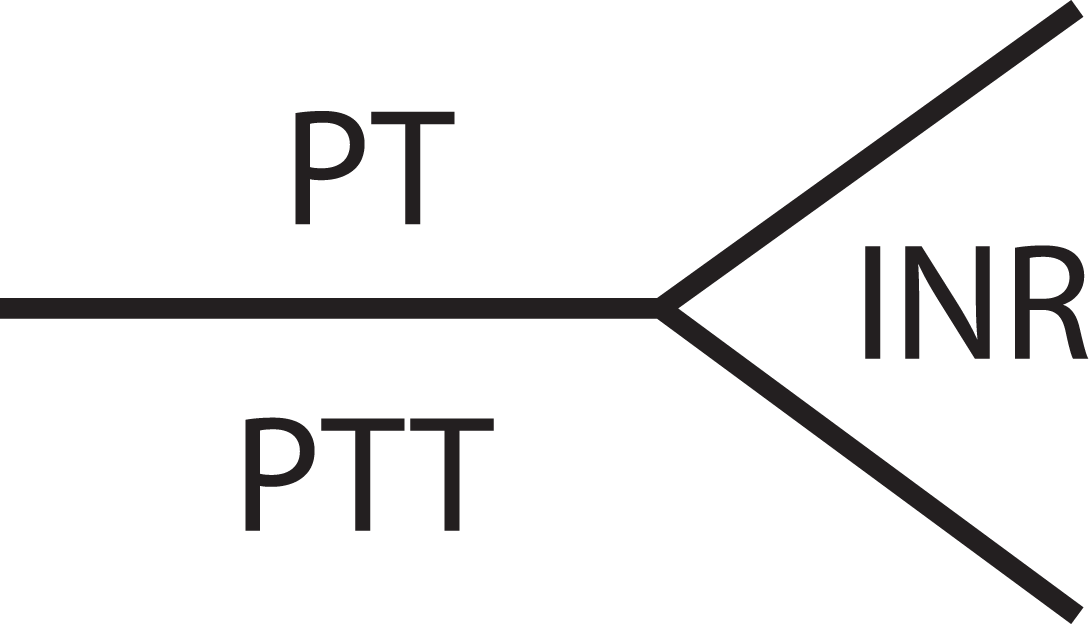
Coagulation:
Protime: 10.9-13.3 sec
INR: 1.0 (a) (when patient is on anticoagulant therapy, such as heparin or warfarin)
PTT: 25.9-35.3 sec
Coagulation - the process of blood clotting that prevents excess blood loss
Clotting factors - many are present in the plasma
Serum - fluid portion of blood MINUS the clotting factors
Fibrin - long, insoluble thread-like protein strand that forms a mesh to trap platelets; formed from soluble fibrinogen molecules during clotting
Coagulation time - the time it takes for clotting to take place when blood is removed from the body
Normal coagulation time - 2-6 minutes
Complete activity 1 using the Gateway Access Virtual Lab: Microscopy (look at a prepared slide of blood).
Complete activity 2 using the Carolina Biological Lab Kit sent to you. You need to upload pictures showing your results. Place your results in Table 20.3.
Look at Exhibit 20.1 on page 241. Highlight the abnormal CBC results.
Complete activity 3 using the image in Figure 20.6 and a ruler. Image a is the normal control. Image b is the test. Put your results in Table 20.5 (Hematocrit Results).
Complete the discussion questions for activity 3 on page 244. Complete the "Reviewing Your Knowledge" questions on pages 245-248. Use the tables throughout the exercise to refer to in answering the questions.
The CBC is a vital diagnostic tool that screens for abnormalities in the number or structure of red blood cells and includes the following components:
- Total red blood cell count
- Total white blood cell count
- Total platelet count
- Differential white blood cell count
- Hematocrit - % of red blood cells in a whole blood sample centrifuged in a capillary tube to pack the RBC's at the outer end of the tube and to separate them from WBC's, platelets and plasma
- Females: normal: 38-46%
- Males: normal: 40-54%
- High: >65% (polycythemia)
- Low: <38% for F or <40% for M (anemia)
- Hemoglobin concentration - protein that carries oxygen in the red blood cells, so this determines that oxygen-carrying capacity of the blood
- Normal: 12-15 g Hb per 100 mL of blood in F
- Normal: 13-16 g Hb per 100 mL of blood in M
- Severe anemia: <7 g Hb per 100 mL of blood
- Closely related to the hematocrit, with a general ratio of 3:1
The differential WBC count is performed to determine the actual percentage of each of the five types of WBC's in a blood sample. Elevations or depressions in these numbers can indicate various diseases, illnesses, or conditions that need to be further evaluated.
CBCWBCRBCHGBHCTMCVMCHMCHCRDWPLTMPVNEUT%LYMPH%MONO%EO%BASO%NEUT#LYMPH#MONO#EO#BASO#4.5-11.0
4.70-6.1014-1842-5283-9928-3431-3711-15.5150-4507.4-10.449-9022-51.10-130-70-31.5-7.06.70-3.00-1.40-0.80-0.3
x 103/UL
x 106/UL
G/DL%FLPG
%%x 103/UL
FL%%%%%x 103/UL
x 103/ULx 103/ULx 103/ULx 103/UL
Coagulation:
Protime: 10.9-13.3 sec
INR: 1.0 (a) (when patient is on anticoagulant therapy, such as heparin or warfarin)
PTT: 25.9-35.3 sec
Coagulation - the process of blood clotting that prevents excess blood loss
Clotting factors - many are present in the plasma
Serum - fluid portion of blood MINUS the clotting factors
Fibrin - long, insoluble thread-like protein strand that forms a mesh to trap platelets; formed from soluble fibrinogen molecules during clotting
Coagulation time - the time it takes for clotting to take place when blood is removed from the body
Normal coagulation time - 2-6 minutes
Complete activity 1 using the Gateway Access Virtual Lab: Microscopy (look at a prepared slide of blood).
Complete activity 2 using the Carolina Biological Lab Kit sent to you. You need to upload pictures showing your results. Place your results in Table 20.3.
Look at Exhibit 20.1 on page 241. Highlight the abnormal CBC results.
Complete activity 3 using the image in Figure 20.6 and a ruler. Image a is the normal control. Image b is the test. Put your results in Table 20.5 (Hematocrit Results).
Complete the discussion questions for activity 3 on page 244. Complete the "Reviewing Your Knowledge" questions on pages 245-248. Use the tables throughout the exercise to refer to in answering the questions.

Here is an unspun (uncentrifuged) tube of whole blood in an EDTA tube.
|

Two tubes of blood are shown here, both collected in EDTA-coated (lavender-top) tubes. In the tube on the left, there are 2 layers because this tube has been centrifuged and has separated into serum (top) and packed RBCs (bottom). This type is a SST (serum separator tube). The tube on the right has not been spun and is whole blood.
|

Two tubes of whole blood collected in an EDTA-coated (lavender-top) tube are shown here. In the tube on the right, which has been sitting for at least 60 minutes, a clot has begun to form. http://www.kingsnake.com/aho/research/srp/mdg2005_1.jpg
|
WHOLE BLOOD: (See images above)
|

Blood ranges from bright red (oxygenated) to dark brick red (deoxygenated) depending upon the hemoglobin level present
|
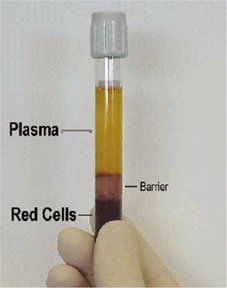
This tube has been centrifuged, so the blood has separated into 3 layers: plasma (top), buffy coat (middle) and red blood cells (bottom; hematocrit)
|

These tubes of blood have been centrifuged and are SST (serum separator tubes), which separate blood into red blood cells and serum
|
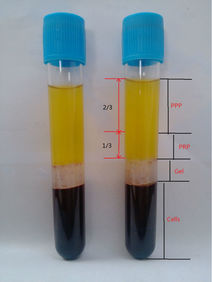
These tubes have been centrifuged and have separated into plasma, buffy coat (white blood cells and platelets) and red blood cells (bottom)
|
COMPONENTS OF BLOOD (CENTRIFUGED) IN AN EDTA ANTICOAGULANT-COATED TUBE: (See images above)
PLASMA
- Fluid portion of blood
- Is the extracellular matrix of blood cells
- Intravascular fluid
- Color: Straw-colored (yellowish)
- Clarity: typically opaque or translucent
- pH: Should range between 7.35-7.45
- Consistency: sticky, due to the presence of clotting factors; slippery (gelatinous)
- Made mostly of water (>90%)
- Contains >100 dissolved substances, including proteins, serum albumins, amino acids, globulins, fatty acids, glucose, vitamins, hormones and fibrinogen
- Protein reservoir
- Contains glucose
- Contains clotting factors
- Factor VIII: used to treat hemophilia A
- Factor IX: used to treat hemophilia B
- Factor X and XIII: used to treat congenital deficiencies
- Immunoglobulin: used to treat immune deficiencies
- Antithrombin III: used to treat disseminated intravascular coagulation (blood clot)
- Fibrinogen: used to treat hemorrhage or congenital deficiency
- C1 inhibitor: used to treat angioedema
- Albumin: used to treat hypoalbuminemia or ascites (fluid)
- Alpha-1-antitrypsin: used to treat emphysema, COPD, liver cirrhosis, congenital deficiency
- Contains electrolytes (sodium, calcium, magnesium, potassium, phosphate, chloride, bicarbonate)
- Contains hormones
- Contains dissolved CO2 gas
- Contains dissolved O2 gas
- Maintains osmosis and osmotic pressure
- Aids in protecting the body from infection
- Can be removed via plasmapheresis and used for treatment during transfusions
- Plasma from AB blood type donors may be collected through apheresis, and with plasma, AB is actually considered to be the "universal donor", unlike whole blood or red blood cell donations, where AB blood type is considered to be the universal recipient
- In some areas a person may be able to donate plasma up to 2x per week
- Plasma regenerates on its own within 48 hours
- Can be frozen (fresh frozen plasma or FFP)
- Fluid portion of blood MINUS the clotting factors
- "Pure blood"
- Leukocytes: white blood cells (WBCs)
- Macrophages
- Neutrophils
- Eosinophils
- Basophils
- T-Lymphocytes
- Helper Cells (help stimulate/activate B-lymphocytes to secrete antibodies called immunoglobulins, of which there are 5)
- Antibodies/Immunoglobulins: IgG, IgA, IgM, IgD, IgE
- IgG: most common and provides the bulk of antibody-antigen immune response against pathogens
- Able to cross the placenta
- Gives passive immunity to the developing fetus
- IgA: found in secretions, saliva, tears, mucus and in breast milk and in mucosal areas of the body like the gut, respiratory tract, urogenital tract; prevents pathogens from colonizing these areas
- IgM: largest; forms complexes; involved in autoimmune diseases
- Stays on the surface of B-cells in monomer form
- Is secreted from B-cells in pentamer form
- IgE: triggers histamine release from mast cells and basophils; plays a role in symptoms of allergies and allergic reactions
- Also fights against parasites and parasitic worms
- IgD: not much is known about it; tends to stay on the surface of the B-lymphocyte
- Activates basophils and mast cells, and plays a role in symptoms of allergies and allergic reactions
- IgG: most common and provides the bulk of antibody-antigen immune response against pathogens
- Antibodies/Immunoglobulins: IgG, IgA, IgM, IgD, IgE
- Cytotoxic Cells (directly kill cancer-infected or virus-infected cells by secreting enzymes that poke holes in the cell membrane)
- Helper Cells (help stimulate/activate B-lymphocytes to secrete antibodies called immunoglobulins, of which there are 5)
- B-Lymphocytes
- Plasma Cells (Antibody-secreting)
- Some memory cells
- Platelets (Thrombocytes): aid in blood clotting, along with clotting factors and vitamin K
- Function: hemostasis (formation of blood clot)
- Packed red blood cells (Erythrocytes)
- Packed red blood cells (PRBCs) may be donated for transfusion, where type O- blood is most desirable since it is the rarest ABO blood type (universal donor)
- AB+ is universal recipient
- Blood with all its components, uncentrifuged/unspun
- May be donated
- Type O- blood is most desirable since it is the rarest ABO blood type (universal donor)
- AB+ is universal recipient
- Donors may typically only donate whole blood once every 8 weeks
- Whole blood cells are returned to the blood
|
CONSTITUENTS OF PLASMA (55%):
|
|
The Formed Elements (Cells) (45%):
Erythrocytes (Red Blood Cells):
http://study.com/cimages/multimages/16/red_blood_cell_ex.png
- Approximately 4-6 million/mm3
- Function: transport of hemoglobin/iron/oxygen to tissues and carbon dioxide away from tissues to be excreted and exhaled
Leukocytes (White Blood Cells):
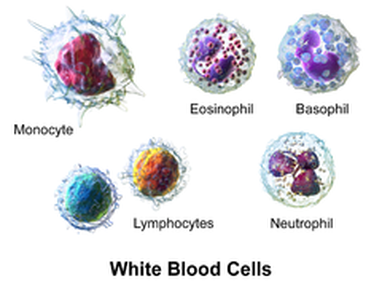
By BruceBlaus. When using this image in external sources it can be cited as:Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. - Own work, CC BY 3.0, https://commons.wikimedia.org/w/index.php?curid=28223981
- Approximately 4,800-10,800/mm3
- Granulocytes: Neutrophils, Eosinophils, Basophils
- Agranulocytes: Monocytes, Lymphocytes
- Function: Immunity and Defense
Platelets:
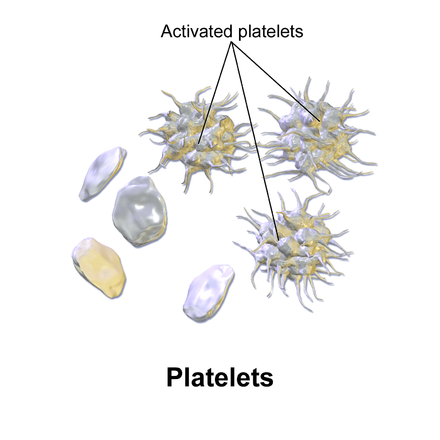
By BruceBlaus. When using this image in external sources it can be cited as:Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. - Own work, CC BY 3.0, https://commons.wikimedia.org/w/index.php?curid=28223979
- Approximately 250,000-400,000/mm3
- Function: Clotting of blood
***Visit https://www.hematologylearning.weebly.com to see all about blood, blood components and blood disorders
Examining Formed Elements Microscopically:
- Please visit https://www.hematologylearning.weebly.com to see images/slides of blood elements (My online hematology atlas)
- Here are a few basic slide images:
Slide: Red Blood Cells (Erythrocytes), White Blood Cells (Neutrohpils, A Lymphocyte and A Monocyte Seen Here), Platelets (Small Purple Spheres Called Thrombocytes)
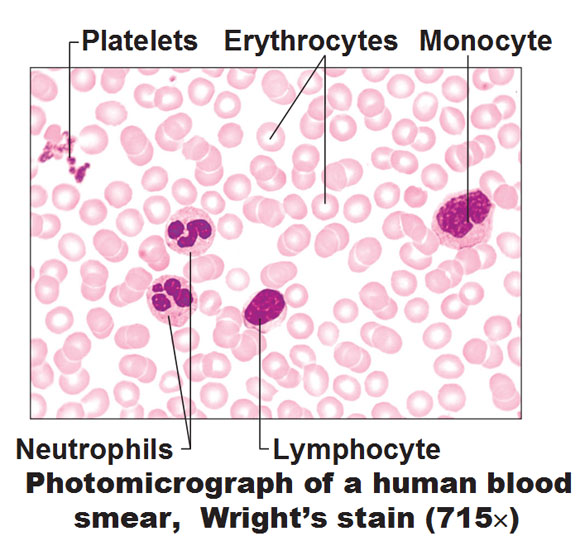
http://antranik.org/wp-content/uploads/2011/12/photomicrograph-of-human-blood-smear-wrights-stain-platelets-erythrocytes-monocyte-neutrophils-lymphocyte.jpg
Examining Red Blood Cells (Erythrocytes) and Platelets (Thrombocytes) (Purple, small, round spheres):
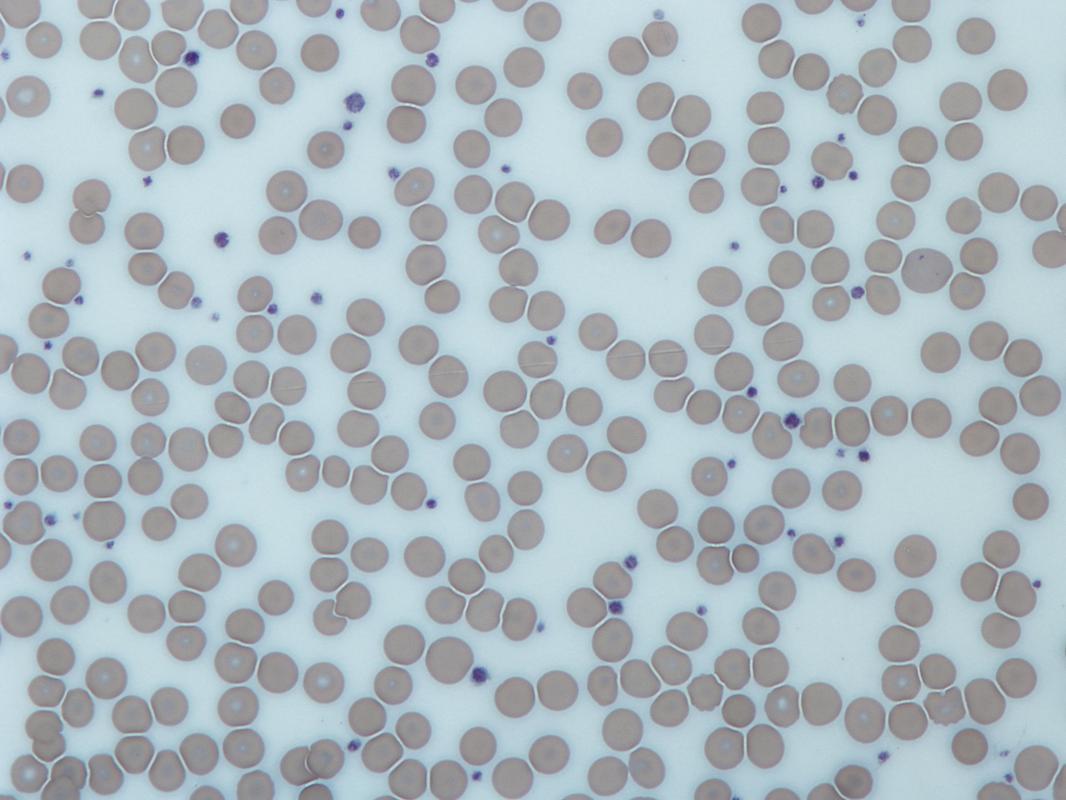
Red blood cells (pink-red) and platelets (purple);By No machine-readable author provided. Graham Beards assumed (based on copyright claims). - No machine-readable source provided. Own work assumed (based on copyright claims)., GFDL, https://commons.wikimedia.org/w/index.php?curid=32208267
Erythrocytes (Red Blood Cells) in Wright's Stain:
https://classconnection.s3.amazonaws.com/225/flashcards/3867225/png/blood-14176A7690009CC7A22.png
ERYTHROCYTES:
- These are the majority of the cells seen on the slide
- They stain pale pink-to salmon red in Wright's stain
- Cells are round-to-slightly oval and average about 7.5 micrometers in diameter
- Cells have a biconcave, disc shape and are slightly paler in the middle than at the edges
- Once mature, red blood cells no longer contain a nucleus
- Red blood cells have a limited lifespan of 100-120 days since they are unable to reproduce
- Red blood cells gradually harden, lose elasticity, and become brittle and less flexible with age and begin to fragment
- Function: Red blood cells carry hemoglobin, a globular, 4-dimensional protein (4 globin chains) containing an iron (Fe) plate in the center, which binds and carries oxygen (O2) throughout the body and delivers it to the tissues of the body
Hemoglobin Molecule:
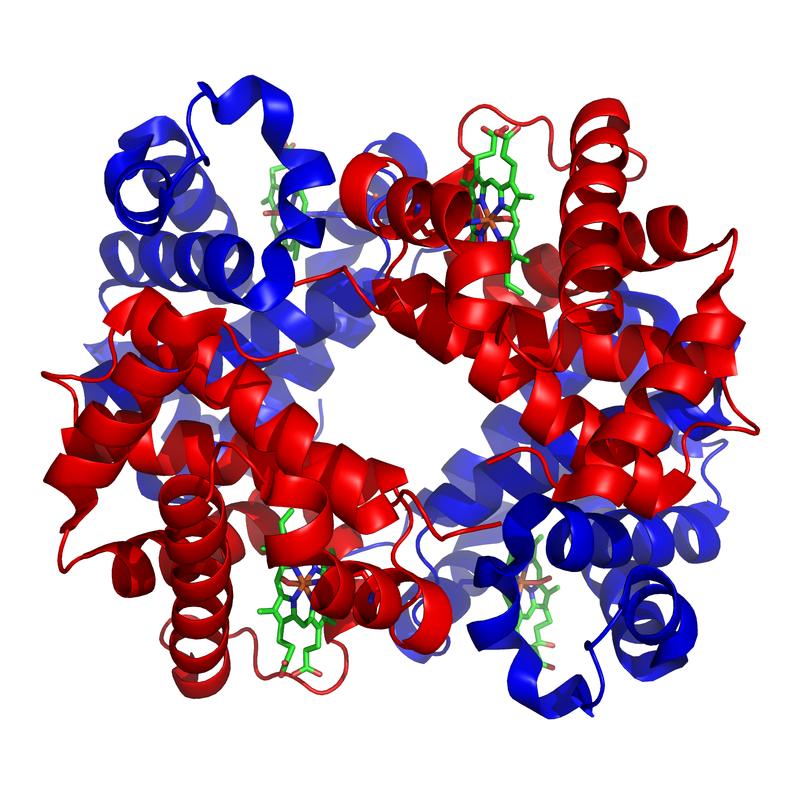
Hemoglobin Molecule;By Zephyris at the English language Wikipedia, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=2300973
|
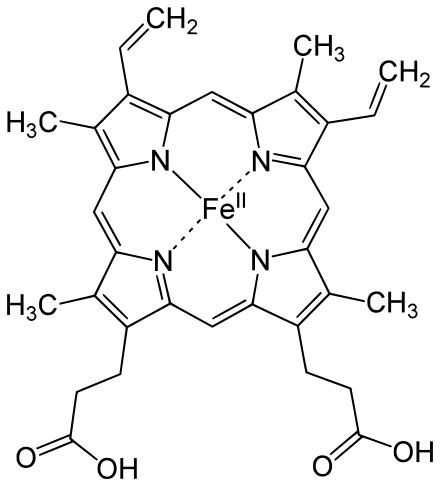
By Yikrazuul - Own work, Public Domain, https://commons.wikimedia.org/w/index.php?curid=11081791
|
LEUKOCYTES:
- White blood cells
- Contain a true nucleus
- Fewer in number than red blood cells
- Protective function
- Destroy disease-causing pathogens
- Transported in blood or lymph to all parts of the body
- Two Major Types:
- Granulocytes
- Contain granules in their cytoplasm that contain potent enzymes for pathogen destruction or contain H2O2 for oxygen burst or contain histamine
- Granule types stain differently with Wright's stain
- Each type has a unique nucleus
- Three Types:
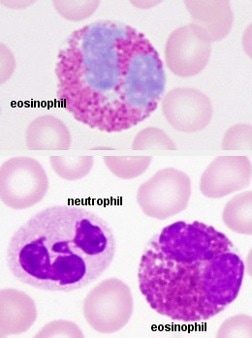
- Neutrophils: neutral loving
- Represent 50-70% of the leukocytes
- Nucleus: 3-5 lobes
- Pale lavender cytoplasm with very fine cytoplasmic granules
- Absorb both acidic (red) stain and basic (blue) stain
- Phagocytes
- Move via chemotaxis
- Increase in number in response to bacterial invasion during acute infection
- Eosinophils:
- Represent 2-4% of the leukocytes
- Bilobed nucleus
- Large cytoplasmic granules that stain red-orange in Wright's stain
- Increase in number in response to parasite infections and during allergies
- Basophils:
- Represent 0.5-1% of the leukocytes
- U-shaped or S-shaped nucleus that is obscured by its coarse, sparse, deep purple granules
- Granules contain histamine, a potent vasodilator that widens blood vessels and mediates the inflammatory response
- Increase in number during major allergic reactions such as anaphylaxis
- Neutrophils: neutral loving
- Agranulocytes
- Do not contain any observable granules in the cytoplasm
- Abundant in the lymphoid tissues
- Sparse in the bloodstream
- Large nuclei that are close to normal in shape and are round, oval, or kidney-shaped
- Two Types:
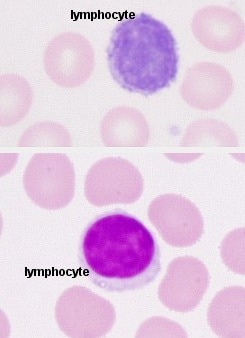
- Lymphocytes:
- Smallest leukocyte representing about 25-45% of the leukocytes
- About the size of a red blood cell
- Large round-to-slightly indented nucleus stains dark blue-to-purple
- Sparse cytoplasm (thin blue ring around nucleus)
- Key role in immunity
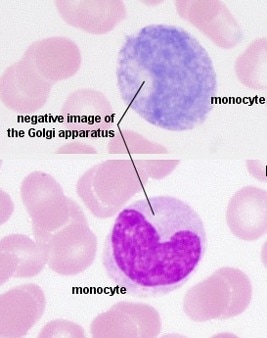
- Monocytes:
- Mature into macrophages
- Largest leukocyte representing about 3-8% of the leukocytes
- About 2x the size of an average red blood cell
- Kidney-shaped nucleus is large and stains dark blue
- Abundant cytoplasm stains gray-blue
- Active phagocyte in immune system
- Increases exponentially during chronic infections and some viruses
- Lymphocytes:
- Do not contain any observable granules in the cytoplasm
- Granulocytes
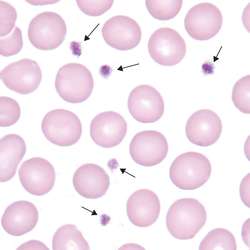
Platelets (Thrombocytes):
- Small spheres of dark purple-staining cell bodies
- May clump or cluster together
- Cell fragments of large, multinucleate ancestral cells referred to as megakaryocytes
- Range from 150,000-400,000/mm3
- Function: form blood clots
- Found in the blood plasma
Granulocytes:
http://www.apsubiology.org/anatomy/2020/2020_Exam_Reviews/Exam_1/granulocytes.bmp
Agranulocytes:
http://www.apsubiology.org/anatomy/2020/2020_Exam_Reviews/Exam_1/lymphocytes.bmp
|
http://www.apsubiology.org/anatomy/2020/2020_Exam_Reviews/Exam_1/monocytes.bmp
|
Platelets:
http://img.tfd.com/MosbyMD/thumb/platelet.jpg
Megakaryocytes:
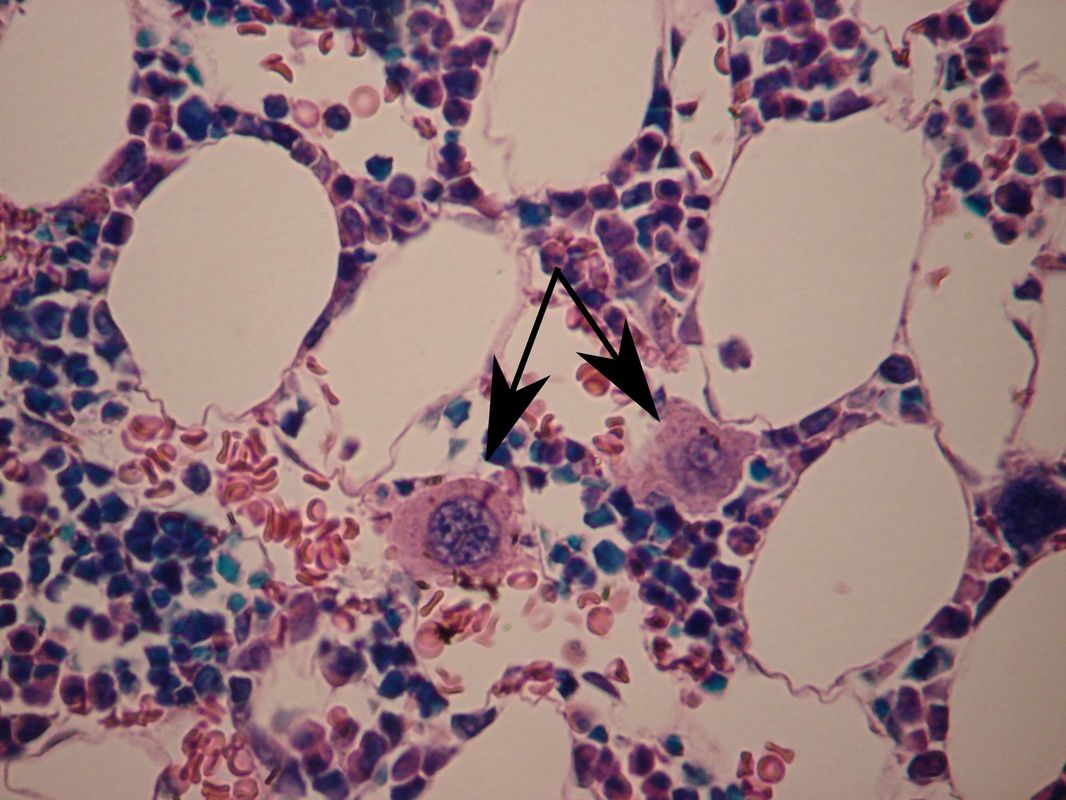
By WVSOM_Megakaryocytes.JPG: Wbensmithderivative work: Icewalker cs (talk) - WVSOM_Megakaryocytes.JPG, CC BY 3.0, https://commons.wikimedia.org/w/index.php?curid=15216382
Some of My Students' Projects:
Tonicity and RBC's:
A 3-D Blood Model:

lood Tests:
Blood Test Type
What it is For
Reference Ranges
Complete Blood Count (CBC)
Diagnostic screening tool for abnormalities in the number of and structure of blood cells.
It includes: total RBC count, platelet count, WBC count, differential WBC count, hematocrit, hemoglobin.
It is used along with blood chemistry tests to put together a comprehensive profile of a person's general level of health based on blood values.
WBC Differential
This is performed to determine the percentage of each of the 5 types of WBC's in a lbood sample.
Elevations or depressions can be indicative of particular diseases or disorders.
Hematocrit (Hct)
This is the percentage of packed RBC's in a whole blood sample that has been centrifued in a capillary tube, separating them from the WBC's and platelets and plasma.
RBC's are measured in length and the percentage is calculated.
Females: 38-46%
Males: 40-54%
Abnormal: >65% (Polycythemia)
Abnormal: <38% F or 40% M (Anemia)
Hemoblogin (Hb)
This protein carries oxygen in the RBC's.
Hb concentration determines the oxygen-carrying capacity of the blood.
Normal: 12-15 g Hb per 100 mL of blood (females)
13-16 g Hb per 100 mL of blood (males)
Severe anemia: <7 g Hb per 100 mL of blood
Normal Hct ratio to Hb in g/100 mL is 3:1
Blood Test Type
What it is For
Reference Ranges
Complete Blood Count (CBC)
Diagnostic screening tool for abnormalities in the number of and structure of blood cells.
It includes: total RBC count, platelet count, WBC count, differential WBC count, hematocrit, hemoglobin.
It is used along with blood chemistry tests to put together a comprehensive profile of a person's general level of health based on blood values.
WBC Differential
This is performed to determine the percentage of each of the 5 types of WBC's in a lbood sample.
Elevations or depressions can be indicative of particular diseases or disorders.
Hematocrit (Hct)
This is the percentage of packed RBC's in a whole blood sample that has been centrifued in a capillary tube, separating them from the WBC's and platelets and plasma.
RBC's are measured in length and the percentage is calculated.
Females: 38-46%
Males: 40-54%
Abnormal: >65% (Polycythemia)
Abnormal: <38% F or 40% M (Anemia)
Hemoblogin (Hb)
This protein carries oxygen in the RBC's.
Hb concentration determines the oxygen-carrying capacity of the blood.
Normal: 12-15 g Hb per 100 mL of blood (females)
13-16 g Hb per 100 mL of blood (males)
Severe anemia: <7 g Hb per 100 mL of blood
Normal Hct ratio to Hb in g/100 mL is 3:1
Clinical Significance and Hematological Tests:
- When a patient enters the hospital, several common hematological (diagnostic) blood tests may be routinely performed to determine the individual's level of health
- Common materials used: vacuutainer tubes for collection of blood, alcohol pads, cotton swabs, lancets, large bands (rubber)
- CBC: Complete Blood Count
- Average RBC: 4.2-5.4 million cells per cubic millimeter for women
- Average RBC: 4.7-6.1 million cells per cubic millimeter for men
- CBC with Diff (Differentiation): Complete Blood Count with Differentiation (of White Blood Cells)
- Average WBC: 4,800-10,800 cells per cubic millimeter
Total White and Red Blood Cell Counts and Common Terminology:
Leukocytosis:
- Abnormally high WBC count
- Could indicate a bacterial infection
- Could indicate a viral infection
- May indicate a hemorrhage (loss of blood)
- May indicate drug poisoning
- May indicate chemical poisoning
- Abnormally low WBC count
- Could indicate viral infection like measles, hepatitis
- May indicate liver cirrhosis (alcoholic or non-alcoholic)
- May indicate excessive antibiotic therapy
- May indicate recent X-ray therapy
- Malignant cancer of the white blood cells of the body
- Disorder of the lymphoid tissues
- Uncontrolled cell division of abnormal WBCs
- Decrease of RBCs and platelets
- Different types
- Increase in the number of RBCs
- May be primary or secondary
- Decrease in the number of RBCs
- Decreased ability to carry oxygen due to less RBCs present or RBCs unable to carry as much oxygen due to decrease in size or hemoglobin content or due to RBCs being destroyed
- A person may still be anemic even if their RBC count is normal
- Many different types, including:
- Iron-deficiency (Decreased Amount or Size of RBCs--->Decreased Iron--->Decreased oxygen)
- Pernicious (Vitamin B deficiency, Lack of Intrinsic Factor, or Destruction of Small Intestinal Microvilli)
- Hemolytic (RBC lysing/destruction)
- Examples: Transfusion reaction, Trauma, Blood Mismatch Resulting in Transfusion Reaction, Rh- Mom Carrying Rh+ Fetus Resulting in Hemolytic Disease of the Newborn
- Sickle Cell (Abnormal Hemoglobin Results in Sickling of Cells)
- Aplastic (Blood Cancer Affecting All 3 Lines of Cells)
- Thalassemias (Group of Anemias Caused by Genetic Disorders)
- Abnormal increase in the number of platelets
- Blood clot or increased risk for
- Abnormal decrease in the number of platelets
- Hemorrhage or increased risk of hemorrhage
Hematocrit:
- This is a test performed when anemia is suspected
- Centrifuge a tube of whole blood in a heparinized capillary tube sealed with clay in a balanced microhematocrit centrifuge
- Formed elements on the bottom (packed red blood cells) = hematocrit (equal to red blood cell volume)
- Average value: Male: 42-52%
- Average value: Female: 37-47%

|

|
Hemoglobin Concentration:
- A way to measure oxygen-carrying capacity
- Average values: Men: 13-18 g
- Averages values: Women: 12-16 g
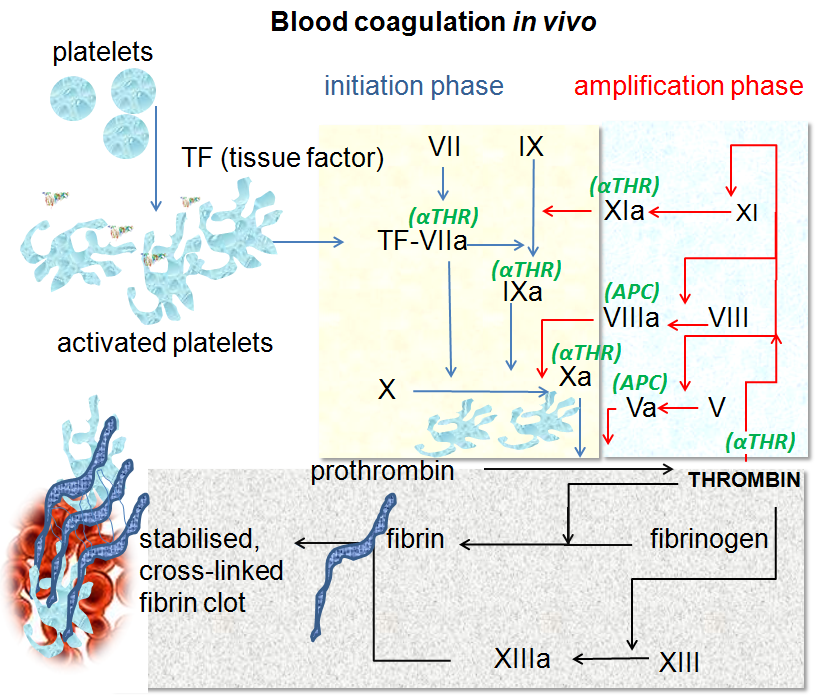
Coagulation Time:
- Coagulation: blood clotting process (hemostasis)
- This is a cascade that minimizes blood loss when blood vessels are cut or injured
- When tissues are injured or ruptured, platelets release something called tissue factor (TF) and platelet factor (PF), which trigger the cascade of coagulation, and they also interact with the other blood clotting factors and calcium ions, forming prothrombin activator, which converts prothrombin (plasma) into thrombin, which polymerizes fibrinogen (plasma) into fibrin, forming a meshwork of strands that traps RBCs and forms a platelet plug or a clot
- Blood collected in a tube clots within 2-6 minutes on average, or 5-15 minutes total (See image above by whole blood)
Coagulation Time:
The process of blood clotting is called coagulation. This prevents excessive blood loss. Many blood clotting factors are present in the plasma. Others are released if there are injured blood vesels and tissues. Platelets initiate the chemical chain reaction to form a blood clot.
Fibrin (long, insoluble, thread-like protein straind) forms a mesh to trap platelets and red blood cells. Fibrin is formed from soluble fibrinogen molecules during clotting.
Coagulation time is the time it takes for clotting to take place when blood is removed from the body. This ranges from 2-6 minutes to 30 minutes to 60 minutes to form a complete clot.
Complete Activity 3 using the Complete Blood Count Form (Exhibit 20.1) and Hematocrit Percentage and Hemoglobin Concentration (Table 20.4). NOTE: This patient is a male.
Calculate the hematocrit for blood in the capillary tubes shown in Figure 20.6, using a millimeter ruler and record in Table 20.5. First, measure the entire column. Second, measure the length of just the packed RBC's. Third, calculate the percentage of RBC's using this formula: length of RBC's in mm/length of entire column in mm x 100. Record the hematocrit in Table 20.5.
Read Table 20.6 to see the significance of elevated and depressed WBC's. Use the tables and figures and exhibits from this entire exercise to complete the discussion questions for activity 3 on page 244 and reviewing your knowledge on pages 245-248.
The process of blood clotting is called coagulation. This prevents excessive blood loss. Many blood clotting factors are present in the plasma. Others are released if there are injured blood vesels and tissues. Platelets initiate the chemical chain reaction to form a blood clot.
Fibrin (long, insoluble, thread-like protein straind) forms a mesh to trap platelets and red blood cells. Fibrin is formed from soluble fibrinogen molecules during clotting.
Coagulation time is the time it takes for clotting to take place when blood is removed from the body. This ranges from 2-6 minutes to 30 minutes to 60 minutes to form a complete clot.
Complete Activity 3 using the Complete Blood Count Form (Exhibit 20.1) and Hematocrit Percentage and Hemoglobin Concentration (Table 20.4). NOTE: This patient is a male.
Calculate the hematocrit for blood in the capillary tubes shown in Figure 20.6, using a millimeter ruler and record in Table 20.5. First, measure the entire column. Second, measure the length of just the packed RBC's. Third, calculate the percentage of RBC's using this formula: length of RBC's in mm/length of entire column in mm x 100. Record the hematocrit in Table 20.5.
Read Table 20.6 to see the significance of elevated and depressed WBC's. Use the tables and figures and exhibits from this entire exercise to complete the discussion questions for activity 3 on page 244 and reviewing your knowledge on pages 245-248.
By Dr Graham Beards - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=19772662

Blood for coagulation tests are collected in the blue-top (citrate) Vacutainer tube;By Gene Hobbs - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=45569646
|
By Elliott.jd - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=20239254
|

Clot formed during the prothrombin time test;By Dietzel65, Steffen Dietzel - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=10206248
|
Blood Typing:
ABO Blood Typing/Classification:
ABO Blood Groups:
Rh (D) Blood Typing/Classification:
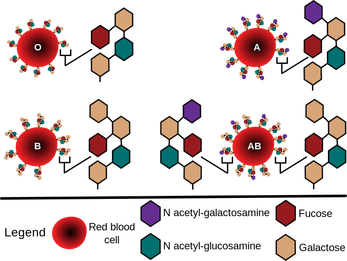
- This is the ABO system of classifying blood based on the presence or absence of glycoprotein receptors on the surface of the red blood cell plasma membrane
- Glycoprotein receptors on the surface of the RBC plasma membrane are called antigens (agglutinogens)
- These are accompanied by plasma proteins called antibodies (agglutinins)
- These antibodies will act against RBCs carrying antigens that do not match the recipient's blood antigens on their own RBCs
- Donor blood must match recipient blood
- If donor blood does not match recipient blood, the recipient's plasma antibodies will attack and react with the donor's RBC antigens, causing them to clump/stick together (agglutinate) and lyse/burst/explode, a phenomenon referred to as a transfusion reaction, which will happen immediately and the first time (upon first exposure to a foreign antigen)
- This is why blood must be carefully typed prior to a blood transfusion
ABO Blood Groups:
- Type A
- A antigens present on RBC membranes
- Anti-B antibodies present in plasma
- 40% of Caucasian, 27% of African American, 28% of Asians in USA
- Type B
- B antigens present on RBC membranes
- Anti-A antibodies present in plasma
- 11% of Caucasian, 20% of African American, 27% of Asians in USA
- Type AB
- Both A and B antigens present on RBC membranes
- No anti-A or anti-B antibodies present in plasma
- Rarest blood type
- 4% of Caucasian, 4% of African American, 5% of Asians in USA
- "Universal Recipient"
- Type O
- Neither A nor B antigens present on RBC membranes
- BOTH anti-A AND anti-B antibodies present in plasma
- Most common blood type
- 45% of Caucasian, 49% of African American, 40% of Asians in USA
- "Universal Donor"
Rh (D) Blood Typing/Classification:
- Rh-positive (+) (D) individuals are those whose cells carry the Rh antigen
- About 85% of the total population in the USA
- Rh-negative (-) (D) individuals are those whose cells lack the Rh antigen
- About 15% of the total population in the USA
- The blood plasma does not carry pre-formed anti-Rh antibodies (unlike the ABO blood group)
- If an Rh-negative individual receives a transfusion of Rh-positive blood, they will become sensitized by the Rh antigens of the Rh- positive donor RBCs, and their own bodies will start to produce anti-Rh antibodies (anti-D) against those antigens
- This means that the next time they receive Rh-positive blood, and every time thereafter, a transfusion reaction will occur, resulting in the clumping and destruction of donor red blood cells (hemolysis)
- If an Rh-negative pregnant female is carrying an Rh-positive fetus, the exact same scenario will happen.
- The first pregnancy will be OK as the Rh-negative female will become sensitized by the Rh antigens of the Rh-positive fetus's RBCs, however, the next pregnancy and every pregnancy thereafter, if she does not receive RHOGAM injections, her RBCs will produce anti-Rh antibodies (anti-D) against the Rh-positive antigens (D), which can cause hemolytic disease of the newborn
ABO Blood Group Classification:
By InvictaHOG - Own work, Public Domain, https://commons.wikimedia.org/w/index.php?curid=1088507
|
By InvictaHOG - Own work, Public Domain, https://commons.wikimedia.org/w/index.php?curid=1161572
|
The Genetics of ABO Blood Type:
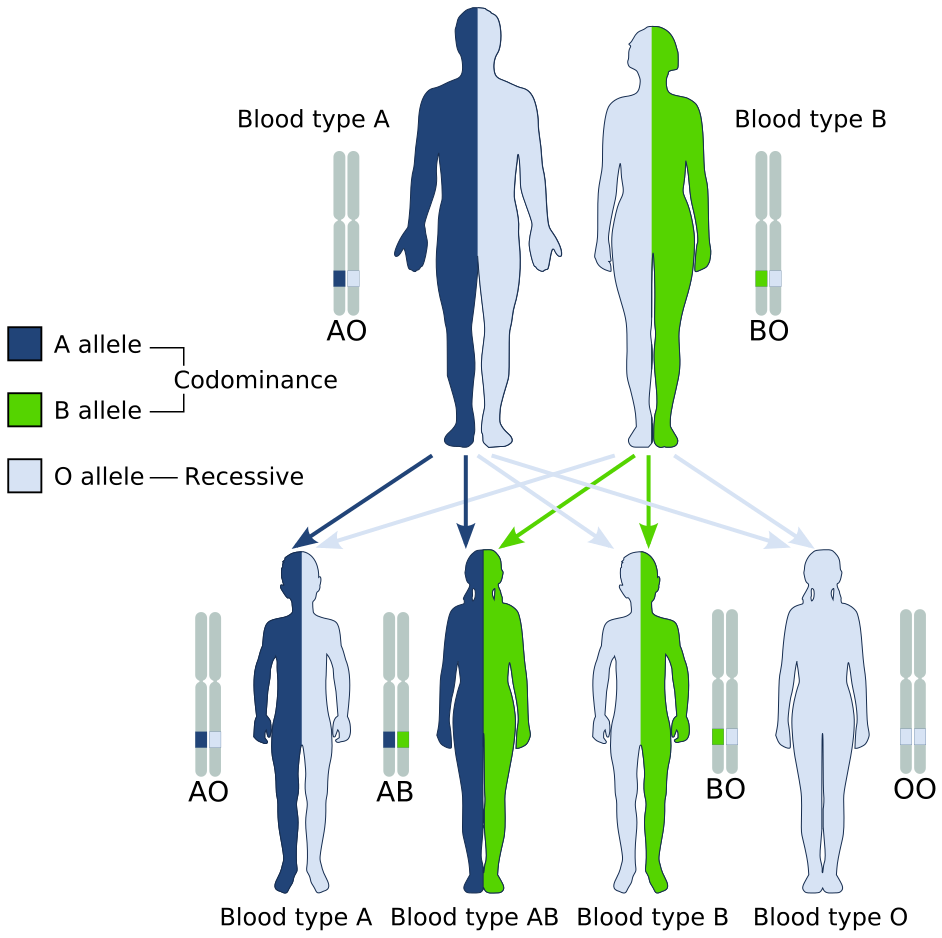
By GYassineMrabetTalk✉This vector image was created with Inkscape. - Own work based on Codominant.jpg, Public Domain, https://commons.wikimedia.org/w/index.php?curid=8395318
ABO and Rh (D) Blood Test:
https://www.biologycorner.com/resources/blood-type-analysis.png

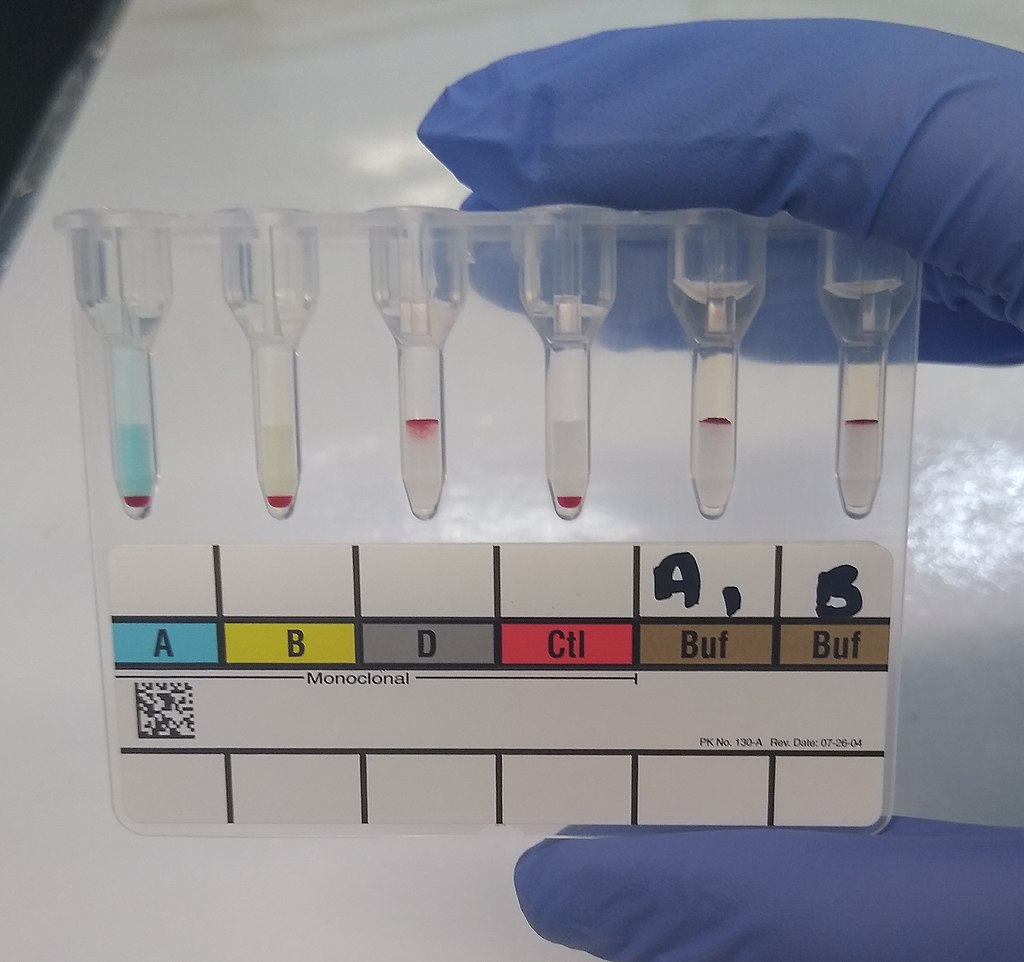
A blood-typing (compatibility) test can be performed on a card (immunoassay), in a tube or in a gel card. There are many different brands and types. The images above reveal the immunoassay card test first, tube test second, and gel card third. The principle behind this is testing the unknown sample (blood) with reagents containing latex-coated antibodies that will react and link with antigens in the patient's blood, resulting in visible clumping (agglutination). It is important for a person to know their blood type in case they should ever need a blood transfusion. Before a transfusion is started, an individual is always cross-matched for compatible blood, in order to reduce the risk for a blood transfusion reaction, which can be deadly. Agglutination causes red blood cells to stick together and clump inside the body in blood vessels, which can damage vessels and organs. It can also cause the cells to burst and lyse (hemolysis).
Antibody screens and identification use reagent containing antigens and if the individual's blood contains antibodies against them, visible clumping will result. An individual's cells can also be cross-matched with donor plasma to detect incompatibilities. Routine blood-typing tests for the ABO blood type and the RhD (Rh factor). This testing involves detection and identification of ABO antigens present on red blood cells (or not) (forward typing), as well as ABO antibodies present in plasma (reverse typing). Blood compatibility testing is performed on pregnant women and cord blood from the newborn, and it is performed when there has been significant blood loss due to trauma or injury, prior to a possible blood transfusion.
Antibody screens and identification use reagent containing antigens and if the individual's blood contains antibodies against them, visible clumping will result. An individual's cells can also be cross-matched with donor plasma to detect incompatibilities. Routine blood-typing tests for the ABO blood type and the RhD (Rh factor). This testing involves detection and identification of ABO antigens present on red blood cells (or not) (forward typing), as well as ABO antibodies present in plasma (reverse typing). Blood compatibility testing is performed on pregnant women and cord blood from the newborn, and it is performed when there has been significant blood loss due to trauma or injury, prior to a possible blood transfusion.
Transfusion Reactions:
- Anaphylactic shock
- Acute hemolytic reactions
- Delayed hemolytic reactions
- Febrile nonhemolytic reactions
- Allergic transfusion reactions
- Post-transfusion purpura
- Transfusion-related acute lung injury
- Transfusion-related circulatory overload (TACO)
- Transfusion-related Graft-Versus-Host Disease (GVHD)
Rh-Negative Pregnant Female Carrying Rh-Positive Fetus:
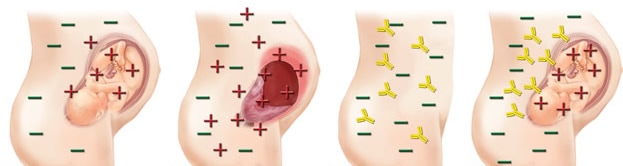
http://biology-forums.com/gallery/14755_16_10_12_12_29_18_9451500.jpeg
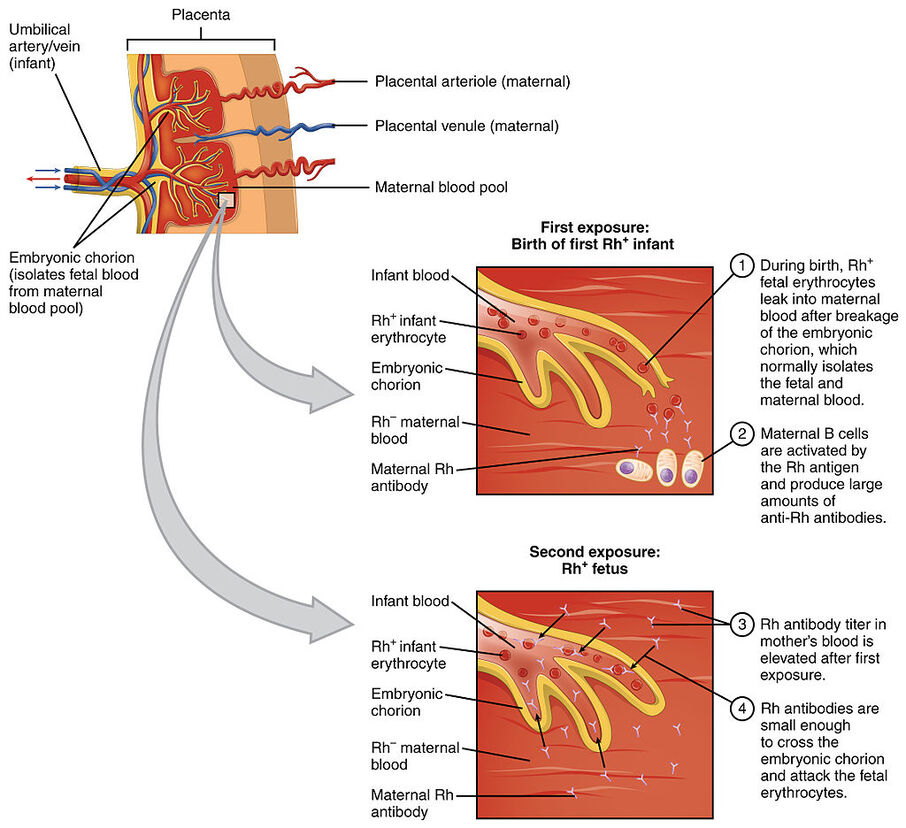
- If mom is RhD- and the fetus is RhD+, the first pregnancy, nothing will happen but she will begin producing antibodies in her plasma (sensitization)
- Second and subsequent pregnancies: The antibodies formed during the first pregnancy put the Rh+ infant at risk of being attacked by the antibodies formed in mom's plasma during her first pregnancy. She will need to take Rhogam shots to prevent this from occurring.
- Without prevention, the infant is at risk for hemolytic disease of the newborn
Hemolytic Disease of the Newborn:
Hemolytic Disease of the Newborn, or erythroblastosis fetalis, is an immune system reaction in which there is blood incompatibility between the mother and the newborn baby. The red blood cells burst open, releasing hemoglobin (pigment), and this can damage the liver and other organs. When the Rh- mother mates with an Rh+ father, and the baby is Rh+, this incompatibility occurs if the Rh+ infant's red blood cells cross the placenta into the Rh- mother's plasma. This typically occurs during the labor and delivery process, when the placenta detaches from the uterus. However, it can occur at any time during the pregnancy when the two blood types mix (miscarriage, trauma, fall, amniocentesis, chorionic villi sampling).
The mother's immune cells do not recognize the baby's Rh+ cells, and see them as "foreign", so they mount an immune response attack against them. She forms antibodies against the antigens (Rh) present on the infant's red blood cells. This happens during second and subsequent pregnancies. The antibodies stay in the mother's plasma circulation in case they are needed in the future. They cross the placenta, and can attack the infant's RBC's in the womb. If it occurs during the pregnancy, it is referred to as erythroblastosis fetalis. If it occurs after the baby is born or during the labor and delivery process, it is called hemolytic disease of the newborn.
As the infant's red blood cells are destroyed, they burst (lyse) in what is called "hemolysis". The infant becomes very anemic and lacks oxygen, resulting in weakness, fatigue, shortness of breath, cyanosis (blue color of the lips and nails), and jaundice of the liver. The liver and spleen can enlarge, causing pain and discomfort. Symptoms range from mild to severe. Mild symptoms include jaundice, mild anemia, and hyperbilirubinemia. Severe anemia results in liver and spleen enlargement. Hydrops fetalis is a major complication in which the anemia is so severe that it puts too much pressure on the baby's immature organs, especially the heart, and they go into heart and organ failure. As fluid builds up, there is a risk of miscarriage or stillborn birth during pregnancy. If hyperbilirubinemia is severe, it is called kernicterus, in which bilirubin can build up in the brain, which can be deadly, or can result in brain damage, deafness, or seizures.
Signs and symptoms to be aware of include:
The mother's immune cells do not recognize the baby's Rh+ cells, and see them as "foreign", so they mount an immune response attack against them. She forms antibodies against the antigens (Rh) present on the infant's red blood cells. This happens during second and subsequent pregnancies. The antibodies stay in the mother's plasma circulation in case they are needed in the future. They cross the placenta, and can attack the infant's RBC's in the womb. If it occurs during the pregnancy, it is referred to as erythroblastosis fetalis. If it occurs after the baby is born or during the labor and delivery process, it is called hemolytic disease of the newborn.
As the infant's red blood cells are destroyed, they burst (lyse) in what is called "hemolysis". The infant becomes very anemic and lacks oxygen, resulting in weakness, fatigue, shortness of breath, cyanosis (blue color of the lips and nails), and jaundice of the liver. The liver and spleen can enlarge, causing pain and discomfort. Symptoms range from mild to severe. Mild symptoms include jaundice, mild anemia, and hyperbilirubinemia. Severe anemia results in liver and spleen enlargement. Hydrops fetalis is a major complication in which the anemia is so severe that it puts too much pressure on the baby's immature organs, especially the heart, and they go into heart and organ failure. As fluid builds up, there is a risk of miscarriage or stillborn birth during pregnancy. If hyperbilirubinemia is severe, it is called kernicterus, in which bilirubin can build up in the brain, which can be deadly, or can result in brain damage, deafness, or seizures.
Signs and symptoms to be aware of include:
- A yellowish color to the amniotic fluid versus clear
- Ultrasound reveals enlarged liver, spleen, fluid buildup around the heart, abdomen, lungs or scalp during the pregnancy
- The newborn infant has pale, yellowish, or bluish coloring due to lack of oxygen, anemia, and/or bilirubin buildup
- Severe swelling all over and difficulty breathing in the newborn infant
- Blood work
- Blood typing and antibody typing and identification on both mom and the infant's umbilical cord blood
- Ultrasound
- Amniocentesis
- The infant is tested for bilirubin levels
- Testing and blood type
- Rhogam shots (second and subsequent pregnancies if the baby is Rh+)
- 1st dose: Around week 28 of the pregnancy
- 2nd dose: Within 72 hours of birth
- 1st dose: Around week 28 of the pregnancy
- Possible blood transfusion or intrauterine blood transfusion
- Early delivery
- IV fluids
- Oxygen
- Exchange transfusion
- IV Immunoglobulin
Who Can Donate/Receive Blood?
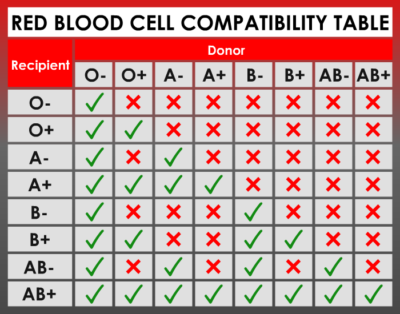
http://qsota.com/wp-content/uploads/2016/11/Blood-type-and-rh-factor-chart.png
Universal Donor: O-
- They can donate/give to any blood type
- They can receive from any blood type
ABO/Rh Blood Typing:
ABO/Rh blood typing is critical for blood transfusions, organ transplants, and maternal-fetal compatibility. It is also used in genetic studies, forensic studies, legal medicine, and anthropology. There are several different types of blood typing, but the most common one is the ABO/Rh blood typing technique.
Blood typing is based on the following criteria:
If you receive the wrong/incompatible blood type, your antibodies will become cross-linked with the antigens present in the blood donation, causing clumping or agglutination, followed by the release of a second plasma protein that attaches to your RBC's and hemolyzes them (causes them to burst), releasing hemoglobin that can cause kidney damage.
ABO antibodies do not cross the placenta because they are too big.
The Rh blood system is different than the ABO system, but contains some similarities.
ABO/Rh blood typing is critical for blood transfusions, organ transplants, and maternal-fetal compatibility. It is also used in genetic studies, forensic studies, legal medicine, and anthropology. There are several different types of blood typing, but the most common one is the ABO/Rh blood typing technique.
Blood typing is based on the following criteria:
- Antigen molecules - agglutinins or agglutinogens found on the surface of the RBC membranes that will react to a specific antibody to produce an immune response. In the ABO system, there are two types of angitens that can be present as surface membrane molecules on RBC's:
- A antigen (type A blood)
- B antigen (type B blood)
- Both A and B antigens together (type AB blood)
- Neither antigen present (type O blood)
- Antibodies - plasma proteins that combine with a specific antigen to inhibit or destroy it. They appear in babies' blood just a few months after birth. Whatever blood type you have, you have its corresponding antibody in your plasma:
- Type A blood (has anti-B antibodies)
- Type B blood (has anti-A antibodies)
- Type AB blood (has neither A nor B antibodies)
- Type O blood (has both anti-A and anti-B antibodies)
If you receive the wrong/incompatible blood type, your antibodies will become cross-linked with the antigens present in the blood donation, causing clumping or agglutination, followed by the release of a second plasma protein that attaches to your RBC's and hemolyzes them (causes them to burst), releasing hemoglobin that can cause kidney damage.
ABO antibodies do not cross the placenta because they are too big.
The Rh blood system is different than the ABO system, but contains some similarities.
- If Rh antigen is present as a surface antigen membrane molecule on your RBC's, you are Rh-positive (+).
- If Rh antigen is not present as a surface antigen membrane molecule on your RBC's, you are Rh-negative (-).
- However, those who are Rh - are not born with the anti-Rh antibody and do not obtain it unless they are exposed to the Rh antigen from Rh + blood during one of the following:
- A blood transfusion
- Sharing a hypodermic needle
- As an Rh - mother carrying an Rh + fetus during the second and subsequent pregnancies
- During delivery, the baby's blood can leak from the placenta into the mother's bloodstream, causing her body to make Rh antibodies.
- The first baby is not affected, but second and subsequent pregnancies with Rh+ fetuses can resulting in the small Rh antibodies crossing the placenta causing hemolysis in the blood of the fetus (hemolytic disease of the newborn).
- Prevention: RhoGAM shots during pregancy and delivery.
- However, those who are Rh - are not born with the anti-Rh antibody and do not obtain it unless they are exposed to the Rh antigen from Rh + blood during one of the following:
References:
The American Red Cross: Facts About Blood and Blood Types: https://www.redcrossblood.org/donate-blood/blood-types.html?icid=rdrt-blood-types&imed=direct&isource=redirect
